
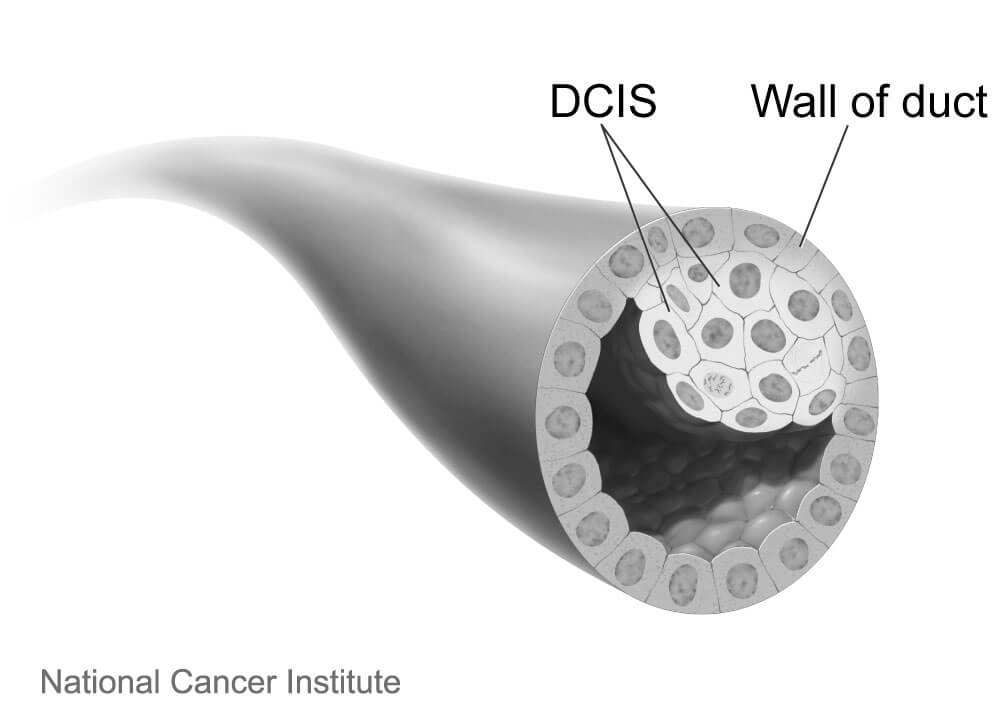
What is ductal carcinoma in situ (DCIS)?
Ductal carcinoma in situ, or DCIS, refers to a type of breast cancer in which the abnormal cells are confined harmlessly within the milk ducts of the breast. Largely due to wide use of mammography screening, about one in five women diagnosed with breast cancer today have this earliest, highly treatable form of the disease.
Is DCIS technically cancer?
Whether DCIS should even be called cancer has been debated, some arguing that the term creates unwarranted anxiety, because it is harmless as long as it remains confined to the milk duct. DCIS cells “are true cancer cells” but the diagnosis should not paralyze people with fear. It is officially termed stage 0 breast cancer.
What are the symptoms of DCIS?
The condition usually doesn’t cause symptoms. A small number of people may have a lump in the breast or discharge (fluid) coming out of the nipple.
How is DCIS diagnosed?
A mammogram can reveal signs of what might be DCIS, and the diagnosis is confirmed by a needle biopsy.
[Learn more about when to get a mammogram.]
What are the treatment options for DCIS?
DCIS is not a life-threatening condition, and no urgent decision about treatment is necessary. It does have the possibility of turning into an invasive cancer, so a person diagnosed with DCIS needs to have a conversation with their physician about what next steps to take.
Once needed, the primary treatment for DCIS is surgery, either a breast-conserving lumpectomy or a mastectomy to remove the lesion and part or all of the breast. Lumpectomy is often supplemented with radiation therapy, and in some cases endocrine (hormone-blocking) therapy is added to forestall a recurrence. Currently, patients treated for DCIS have excellent breast-cancer-specific survival of about 98 percent after 10 years of follow-up and can expect normal longevity.
Examining cells from a biopsy can help pathologists determine if the DCIS is considered low, medium, or high-risk of becoming invasive cancer. There are widespread concerns that many people with low-risk DCIS that is unlikely to become invasive are being overtreated, incurring needless surgeries and potentially long-lasting pain and emotional distress. Whether a person with low-risk DCIS should undergo immediate surgery or could safely delay treatment and be monitored with regular mammograms is an issue being studied in a clinical trial called COMET (Comparing an Operation to Monitoring, with or without Endocrine Therapy). It is the first large-scale comparison of these two approaches for low-risk DCIS.
Ann Partridge, MD, MPH, is the co-principal investigator of COMET, which began in early 2017 and is enrolling 1,200 women age 40 or older who have been newly diagnosed with low-risk DCIS at cancer centers across the United States. The women are randomly assigned to one of two groups: One group will undergo standard treatment with surgery with or without radiation, while women in the other group will be closely monitored with mammograms and will be recommended to have surgery only if invasive cancer is detected. Women in both groups will have the option to take hormonal therapy to reduce risks further.
Expected to be completed in 2023, the COMET study will compare the cancer and quality of life outcomes in the two groups. The results will help doctors and patients determine if women with low-risk DCIS can safely choose to avoid immediate aggressive treatments and rely on active monitoring to watch for signs that the DCIS is becoming invasive.
What happens if DCIS is not treated?
Left untreated, some of these lesions will in time escape through the wall of the ducts, becoming invasive, and then potentially enter the lymph nodes or blood stream, where they can spread to other parts of the body. Other DCIS lesions will never become invasive in the woman’s lifetime. Because the course of DCIS is unpredictable, it is almost always treated to forestall the development of a more risky invasive tumor.
I was diagnosed with DCIS Stage 2 in right breast. Has mastectomy in Feb 2015..2 drains..kinda messy~Also had a small lumpectomy in left breast during same surgery. Path report DCIS 0 – benign. Taking Letrozole, generic for Femara. Oncologist prescribed it. Now, they want to do radiation for left breast, as a precaution for 5 days a week, for 5 or more weeks.New Mammo in June 2015 shows NO microcalcifications, but radiation still recommended. Maternal aunt and her daughter had cancer. Cousin had the lumpectomey with radiation. I’m 75. Radiologist says I should do the BRCA1 & 2 test, as I’m Askenazi Jewish. Went for CT scan June 10, 2015, to get marked for the radiation treatment. Since it’s the left breast, they will do radiation on my back, to avoid heart and lung problems. Just hoping my 2 daughters won’t have to go thru this. They will be 39 and 41 this summer.Good luck and keep positive ladies, there’s a lot of living, laughing, loving and learning ahead!
I’m new to this, was just diagnosed 2 days ago. I myself have Ashkenazi ancestry. Never thought about getting the genetic test to see if there is a mutation in the BRCA genes. Thank you for mentioning this.
I was diagnosed with DCIS stage zero Novemeber 2014. Saw many doctors and they ALL strongly pressured me to have mastectomy. I educated myself on this condition and all the evidence out there, and THIS article is consistent with what I learned and says “chances of dying from DCIS alone is almost ZERO”. Then this article goes on to suggest aggressive, known-to-be HAZZARDOUS “treatments”! Wow! No pink ribbon for me thank you very much. I’m never getting another mammogram unless I feel something is truly and terribly wrong. The stress of all this has likely harmed me more than the DCIS ever will.
I was just diagnosed with DCIS with two spots in my right breast my consult is next week and I’m so confused as to what to do. With a family history of ovarian and breast cancer I am leaning towards removing both breasts without reconstruction surgery. My sister had breast cancer at age 31, my aunt died from ovarian cancer, my other aunt died from breast cancer and had the BRCA 1 gene mutation. I know it’s not considered invasive cancer but I’m pretty sure I don’t want to wait for it to become invasive cancer. Thanks to mammograms they are able to catch DCIS before it becomes invasive. Wow I have read so much and it’s contradicting in itself but why would someone diagnosed even consider ignoring it. Any help would be greatly appreciated.
Dear Tammy —
We are so sorry to hear about your recent health issues. Unfortunately, we cannot give out medical advice over this blog or email. You bring up a lot of important points about family history of disease, and it will be important to discuss this history, as well as any questions you have, with your doctor. Wishing you all the best.
I was diagnosed last week with DCIS. For the past 6 years, I have been seeing a breast surgeon once a year, along with my GYN once a year. Everytime I go for my mammography, it always leads to a follow-up ultrasound due to very dense breasts. I already had a lumpectomy to remove a noncancerous growth back in 2009. I go to see a specialist at Penn tomorrow. I plan to discuss a bilateral mastectomy simply because I am so tired of the red flags that go up time after time due to the density in my breasts and now that they discovered DCIS, I am afraid that it could potentially tun into invasive breast cancer and with my very dense breasts, who knows if they will see it in time! I am really looking forward to hearing what the breast surgeon says tomorrow. Good luck everyone with your decisions!
Sandy, will you update us on your consult at Penn. I know Penn is highly rated but I never know if that refers to U. of Pennsylvania OR Pennsylvania Hospital. Thanks
i just was told i have micro calfications. confused as well. if am i not going to why treated. also, if you treat and biospy is a chance for cells to spread and could cause a recurance. i know of no one not treated and had bad problems.
message for Cornelia; Hi Cornelia, I see what you’re talking about…what did you end up doing and how are you doing? Thanks