
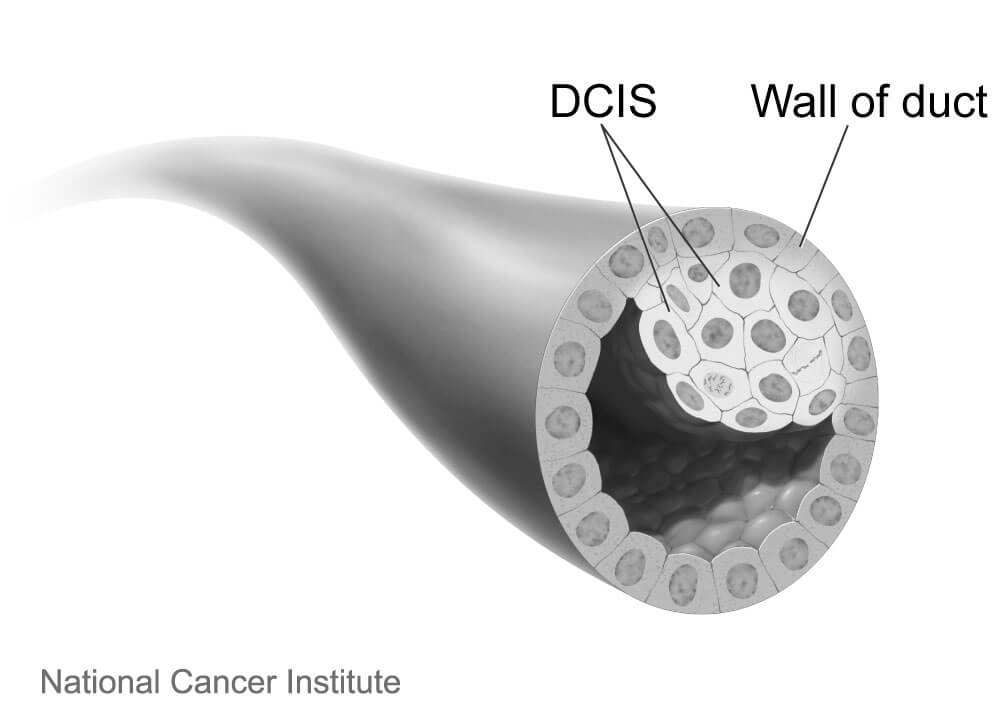
What is ductal carcinoma in situ (DCIS)?
Ductal carcinoma in situ, or DCIS, refers to a type of breast cancer in which the abnormal cells are confined harmlessly within the milk ducts of the breast. Largely due to wide use of mammography screening, about one in five women diagnosed with breast cancer today have this earliest, highly treatable form of the disease.
Is DCIS technically cancer?
Whether DCIS should even be called cancer has been debated, some arguing that the term creates unwarranted anxiety, because it is harmless as long as it remains confined to the milk duct. DCIS cells “are true cancer cells” but the diagnosis should not paralyze people with fear. It is officially termed stage 0 breast cancer.
What are the symptoms of DCIS?
The condition usually doesn’t cause symptoms. A small number of people may have a lump in the breast or discharge (fluid) coming out of the nipple.
How is DCIS diagnosed?
A mammogram can reveal signs of what might be DCIS, and the diagnosis is confirmed by a needle biopsy.
[Learn more about when to get a mammogram.]
What are the treatment options for DCIS?
DCIS is not a life-threatening condition, and no urgent decision about treatment is necessary. It does have the possibility of turning into an invasive cancer, so a person diagnosed with DCIS needs to have a conversation with their physician about what next steps to take.
Once needed, the primary treatment for DCIS is surgery, either a breast-conserving lumpectomy or a mastectomy to remove the lesion and part or all of the breast. Lumpectomy is often supplemented with radiation therapy, and in some cases endocrine (hormone-blocking) therapy is added to forestall a recurrence. Currently, patients treated for DCIS have excellent breast-cancer-specific survival of about 98 percent after 10 years of follow-up and can expect normal longevity.
Examining cells from a biopsy can help pathologists determine if the DCIS is considered low, medium, or high-risk of becoming invasive cancer. There are widespread concerns that many people with low-risk DCIS that is unlikely to become invasive are being overtreated, incurring needless surgeries and potentially long-lasting pain and emotional distress. Whether a person with low-risk DCIS should undergo immediate surgery or could safely delay treatment and be monitored with regular mammograms is an issue being studied in a clinical trial called COMET (Comparing an Operation to Monitoring, with or without Endocrine Therapy). It is the first large-scale comparison of these two approaches for low-risk DCIS.
Ann Partridge, MD, MPH, is the co-principal investigator of COMET, which began in early 2017 and is enrolling 1,200 women age 40 or older who have been newly diagnosed with low-risk DCIS at cancer centers across the United States. The women are randomly assigned to one of two groups: One group will undergo standard treatment with surgery with or without radiation, while women in the other group will be closely monitored with mammograms and will be recommended to have surgery only if invasive cancer is detected. Women in both groups will have the option to take hormonal therapy to reduce risks further.
Expected to be completed in 2023, the COMET study will compare the cancer and quality of life outcomes in the two groups. The results will help doctors and patients determine if women with low-risk DCIS can safely choose to avoid immediate aggressive treatments and rely on active monitoring to watch for signs that the DCIS is becoming invasive.
What happens if DCIS is not treated?
Left untreated, some of these lesions will in time escape through the wall of the ducts, becoming invasive, and then potentially enter the lymph nodes or blood stream, where they can spread to other parts of the body. Other DCIS lesions will never become invasive in the woman’s lifetime. Because the course of DCIS is unpredictable, it is almost always treated to forestall the development of a more risky invasive tumor.
I was diagnosed with DCIS last December and had a left breast mastectomoy. with immediate reconstruction. Did not do chemo, doctors did not feel the need, and I decided not to take the tamoxifen after much thought and discussion with the doctors. Recent mammo was negative and all blood was good. I was very pleased with the treatment at Tufts and the excellent care from all involved.
I had DCIS three years ago. I tried taking the tamoxifen three times. Each time my body would ache all over. I couldn’t even squeeze the shampoo bottle. My Dr. was no help. She said if you can’t take it then I guess you can go off it. I Also had stage II Melanoma six months before. I just hope I never have cancer again because I will have to find another Oncologist. Thanks for the information. I feel better with my decision now.
I dealt with DCIS in 2000. It was not diagnosed as cancer by the specialists I saw in a well-known teaching hospital in northern FL. My late uncle was a retired pathologist and cancer researcher, who sent off copies of my slides to a colleague, who diagnosed DCIS. Based on that diagnosis, I had a lumpectomy (they called it a segmental mastectomy), radiation, & took tamoxifen for several years. I’m happy to report that I have been cancer free since then. I feel like it is best to “call it cancer” and treat it aggressively. I still feel as though my late uncle saved my life! In 2009, I was diagnosed with ovarian cancer. It was easier the second time with cancer, since it was found at an early stage like the breast cancer and knowing that I would do what I had to do for treatment, I had faith that I would have another positive outcome. And I have been recurrence free for the past 4 years…
I was diagnosed 5 years ago with DCIS. Had a lumpectomy, chemo, radiation and Herceptin for a year. Thank God for my oncologist getting me thru all of this. Come march 2014 I hit my 5 year cancer free mark. From the time I had the biopsy to the time I had surgery multiple tumors were found.
I was diagnosed with DCIS in April of 2007. I had a mastectomy /reconstruction and took Tamoxifin for 5 years. I have had two more brushes with cancer- sarcoma and uterine. Dana Farber was there every step of the way for me. I feel blessed to have their expertise and compassion. I only wish insurance would have allowed me the peace of mind to have had a preventative mastectomy on the left breast since I do have calcifications there as well.
Thank goodness! At Last! What has taken them so Long?
Four years ago, I had Invasive Breast Cancer with a
double “breast removal” (I hate the other word!)——-I had Reconstructive at the same time and did Chemo— had extra nodes taken out–a month later—–lost my hair ———etc—-lots of neuropathy now.
At the time and even now I get so upset when I hear so many women calling their Ductual “cancer”
It took me a long time to get in contact with someone who
actually had cancer has I did.
Let’s stop calling non-cancer ———-cancer and please
could we stop calling future treatments “battling the disease.”
Wow Helen. I’m sorry if my cancer isn’t cancer enough for you. It is called cancer because it is cancer. Having it confined at this time to one place doesn’t change the fact that they are cancer cells.
I usually don’t respond to posts but felt I had to. There seems to be confusion as to what DCIS is. I was diagnosed with DCIS in October of 2014. Because I had 2 areas of DCIS, my doctor at Dana Faber told me I was not a good candidate for a lumpectomy because they had to remove too much of my breast. I had a mastectomy and a preventative mastectomy in the other breast- which is covered by insurance. DCIS IS cancer, thankfully non-invasive. While our treatments may not include chemo, we are still losing our breasts, undergoing radiation and taking tamoxifen, something that should not be down played.
Thank you for your post.
Thank you for the comment, I was diagnosed yesterday and was scheduled for surgery Sept 24. I pray that they get it all and it never becomes invasive.
I had DCIS in 2012. I refused a core needle biopsy; why rupture the duct and risk spread. I had a CO2 laser procedure to remove the duct intact. It was pre-cancerous. No further treatment needed since the duct was removed intact. The surgery was 1 hour in office suite with no after pain or swelling. I went out to lunch after it! Why are surgeons still using scalpels when this is available??????? Why would anyone do a core needle biopsy knowing that it risks spread of disease?
Hi Marie. I am 66. I have no family history of breast cancer or any cancers, so very blessed. I skipped my mammogram for 2 years and, lo and behold, this one showed something. My primary sent me to breast surgeon who ordered an MRI and minutes later I was told I needed a needle core biopsy done right then and there, which I was not at all prepared for. I did not know the Doctor or tech that was doing this and I kept asking while crying, why are we doing this as I believe it is only common sense, if it is a contained cancer and you open up a channel for this to escape then it will surely spread. I was only comforted with the words that it is better to know for sure so I can get treatment. I have never had anything so painful as that pushing. Results came back with DCIS so she wants to go in and remove lump. I went to see another breast surgeon, both Doctors are general surgeons specializing in breasts. I did like this Doctor. He contacted the breast clinic that did my biopsy and requested the slides which he sent off to two other places out of state for second and third opinions. The diagnosis did come back the same so now I am faced with this surgery and I do not want to do it. I have never had pain in my breast until after the biopsy which bruised me badly and breast us still sore.. I went in for right mammogram two weeks ago and my old calcifications that were no worry then and have changed very little, are being requested to do the same biopsy. The radiologist came in and told me that these are 95% benign and not to worry but he sent letter to my Dr. stating I need a core biopsy. Please help me as to your procedure of removal of the gland versus the lumpectomy which could easily become a mastectomy after what I have just read. Should a very good breast surgeon know about your CO2 laser procedure and why is this not being done instead of the worst option ? I am considering doing nothing now if I cannot find your laser treatment cause once they start cutting, it never ends. Thanks so much and so happy you are healthy. Patti
Hi patti and Marie,
I am 44 years old and was diagnosed with stage zero dcis back in august of 2012 and A biopsy was done to confirm the disease. Which I now realize May have caused the cells to spread more since my last mammogram done 04/02/2015. I refused treatment which consisted of the removal of my left breast for something I was told was not life threatening and contained. I am very confused and am wondering why that C02 procedure was not offered to me. My concern is why are these doctors offering drastic life changing surgeries for something that is supposed to be non life threatening then doing a biopsy which can help spread the contained diseased cells. All I can think of is that Cancer is a money making disease and the money is in the treatment not the cure. Radiation, chem, and reconstructive surgery are money making procedures. I know because I work at a cancer center. I have not had any treatment as of yet because I have so much confusion regarding this dcis and I just don’t know what to do! Every doctor I see it seems that they try and scare me into the removal of my Breast so that I won’t die later. Why aren’t there any other options. Please help!!!!!!!!! I’m so over it and don’t know what to do next. I’m being told to act now before it is too late the same thing that I was told back in 2012.
How did you find a Doctor who would do CO2 laser procedure.I am looking all over the internet and can’t find one. Any help would be greatly appreciated I am located in Los Angeles CA
OH MY..I had no idea that this procedure was available. To late I have already had a biopsy. We so need to be better informed.
I had a diagnosis of ductal carcinoma in situ (DCIS)– which was not scary to me but I went with a double mastectomy in response. The reason being is that while I agree, this is an extreme surgical response that’s prolly not medically warranted; the bottom line was I felt that the intense medical surveillance required by today’s protocols are alone reason enough to get a mastectomy. A mammogram is no walk in the park, a needle biopsy is worse, and while some may disagree, I found the stereotactic mammogram to be even worse than a lumpectomy. I’ve had all of these “less than” a mastectomy options and I found them all to be taxing & humiliating. Constant breast surveillance (even when the findings are benign) was too much for me. It’s hard enough for me to even write b-r-e-a-s-t. So, I welcomed the DCIS diagnosis as my chance to escape today’s protocols. The surgery is intense. Still I can also say I’m happier with a flat chest (free nipple transplant, too) and the knowledge that I will NEVER have to return for breast surveillance! This is much better than allowing the docs to disfigure and humiliate me bite, by bite, at 6 months intervals. I’m thankful to have made this choice early and avoided a lesser surgery combined with radiation and hormone altering meds.
With my Ductal I had the joy of experiencing a Biopsy … Lumpectomy .. 6 weeks of radiation.. A pretty ugly looking right breast.. The fun of a mammogram every 6 months.. Genetic testing to see if I carry the gene for breast cancer..appointments with my oncologist .. Questions about whether or not I should take tamixifen..If you don’t call that cancer then what do you call it?
In 2007 I was diagnosed with DCIS. Had several core needle biopsies leading up to that, then 2 stereotactic biopsies which were not fun. I had a large lumpectomy and 6 weeks of radiation. The path report showed DCIS had broken through duct in a couple of places. Mine was more extensive than they originally thought. Nonetheless they told me after radiation I would be ok. I put up with the increased surveillance and was declared cancer free and once I made it 5 years they said it would never come back. In 2014 it returned. I had a mastectomy and the path report said not only had dcis returned but I had a new primary large area of dcis. I don’t understand Helen’s remarks at all. It is called cancer because it is cancer. Cancer grows and spreads, and we know that and that is why it is treated. If dcis were not treated we would have a lot of dead women from breast cancer. Call us lucky because it was caught early. If it wasn’t cancer I would still have my breasts!