
Having come to fame as the basis of the Moderna and Pfizer/BioNTech vaccines for COVID-19, messenger RNA — or mRNA — is in many ways the molecule of the moment.
Its newfound prominence is also raising its profile as a powerful tool in cancer research. Scientists are using it learn how cancer cells sometimes disarm the immune system and have developed mRNA vaccines that spur an immune attack on tumors.
Both the COVID vaccines and the cancer studies take advantage of mRNA’s role as a courier of genetic information. Because it acts as an intermediary between the DNA in the genome and the cell’s protein-making machinery, mRNA can tell scientists which genes are active within a cell; and because it carries instructions for protein assembly, it can be harnessed to produce proteins that alert the immune system to the presence of cancer.
Treating COVID, studying cancer
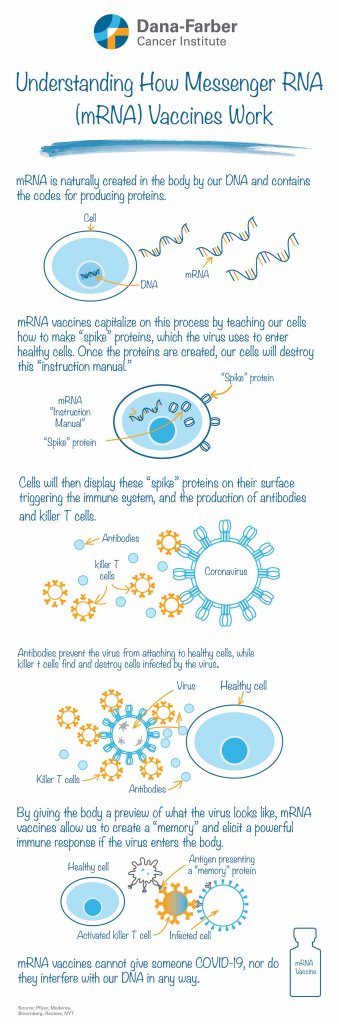
The mRNA vaccines for COVID-19 hold the genetic code for the spike protein that the coronavirus uses to attach to human cells. When a vaccinated person’s cells take up the mRNA, they begin producing the spike, which, by itself, is a harmless protein. The immune system responds to the newly made spikes by generating antibodies against them. Should the person be exposed to the coronavirus, these antibodies as well as immune system T cells are ready to neutralize it and protect the individual from developing COVID.
In cancer, mRNA is helping researchers study the disease as well as treat it.
With new technology, scientists can detach individual cells from a tumor — cancer cells as well as neighboring immune system cells — and analyze the mRNA within them. The collection of mRNAs indicates which genes are active within the cell and which are idle.
“For the immune system cells within the tumor, this lets us understand how the cells are ‘wired,’ how they’re programmed to function,” says Dana-Farber’s David Braun, MD, PhD, a physician-scientist who specializes in immunology and kidney cancer.
In a recent pair of studies in the journal Cancer Cell, Braun and his colleagues used this technique to explore how the immune cells within kidney tumors change as tumors form, grow larger, and eventually metastasize.
“We showed that the immune cells were becoming more and more dysfunctional,” Braun says. “By noting changes in their mRNA, we could track how different immune cells were communicating with each other. We found that some cells, called macrophages, were issuing instructions that caused T cells to become ‘exhausted,’ or less active against tumor cells. The T cells, meanwhile, were sending messages that supported these abnormal macrophages. It was a vicious cycle that resulted in weakening the immune response to the cancer.”
The findings may suggest ways of intervening in this intercellular exchange to re-energize the immune response. “Now that we have a map of the circuitry among the cells, we may be able to break the circuit at strategic points to restore immune function,” Braun remarks.
In a similar avenue of investigation, Dana-Farber’s Eliezer Van Allen, MD, and his colleagues conducted an mRNA analysis to explore how populations of immune cells shift in response to immunotherapy in patients with advanced kidney cancer. Among their findings: certain types of T cells are more numerous in patients who had received the therapy.
Treatment vaccines
Unlike mRNA vaccines for COVID-19, mRNA vaccines for cancer are meant to treat the disease, not prevent it. Beyond that, however, they’re based on the same principle: use mRNA molecules to trigger the production of proteins that rouse the immune system to attack a foreign invader such as the coronavirus, or an abnormal cell such as a tumor cell.
Dana-Farber’s Patrick Ott, MD, PhD, is leading the Institute’s participation in a clinical trial of one such vaccine, produced by BioNTech, for patients with certain types of cancer.
For all its utility, mRNA represents just one route to a cancer vaccine. The personalized NeoVax vaccine developed by Catherine Wu, MD, and colleagues at Dana-Farber and the Broad Institute of MIT and Harvard, is made of peptides, protein fragments unique to each patient’s tumor. By identifying these peptides in a patient’s tumor sample, copying them in a lab, and injecting them into the patient as a vaccine, physicians have been able to provoke a potent immune response to multiple types of cancer. Combining NeoVax with immune checkpoint inhibitor drugs, which remove some of the impediments to an immune attack on cancer, may enhance the vaccine’s effectiveness. With Ott and Toni Choueiri, MD, Braun is leading the first clinical trial of NeoVax in patients with kidney cancer.
Has there been any progress in treating SCLC. / 3A with the new technology of mRNA?
Hi Patricia,
Thank you for reading. So far, there has not been a lot of progress in terms of mRNA for SCLC. You can learn more about treatment for small cell lung cancer here, as well as other advancements: https://www.dana-farber.org/small-cell-lung-cancer/
Wishing you the best,
DFCI
Could combination of CAR therapy and mRNA vaccine be more effective than one alone ?
Hi Suheil,
Thank you for reading. The BioNTech team (behind the Pfizer COVID vaccine) has actually already started to explore this, and published an initial study in Science last year (https://science.sciencemag.org/content/367/6476/446).
Wishing you all the best,
DFCI